AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-8808/017
1* St.George Clinic of Thorasic and Cardiovascular Surgery, Pirogov National Medical and Surgical Center, the Russian Federation, Moscow.
*Corresponding Author: Shevchenko Yury Leonidovich, St. George Clinic of Thorasic and Cardiovascular Surgery, Pirogov National Medical and Surgical Center, the Russian Federation, Moscow.
Citation: Shevchenko Y Leonidovich, Ermakov D Yuryevich, Vahrameeva A Yuryevna, (2020) Orthostatic Hypotension in a Complex Clinical Setting Use of the Heart Rate Increase/Systolic Blood Pressure Decrease Ratio as a Diagnostic Aid. J Clinical Case Reports and Studies, 1(6): Doi: 10.31579/2690-8808/017
Copyright: © 2020. Shevchenko Yury Leonidovich. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 July 2020 | Accepted: 20 July 2020 | Published: 19 September 2020
Keywords: electrocardiography; ECG of the coronary sinus; bifurcational lesion of the coronary arteries; control of ischemia of myocardium
Introduction: The aim of this investigation is to evaluate the possibilities of the method of cardiography from the coronary sinus (ECG-CS) in optimization of stenting bifurcation lesions (BL) of coronary arteries (CA).
Materials and Methods: 43 patients with stable CHD with pseudo-BL of the anterior descending artery (ADA) were included in this investigation. We placed a 10-canal electrode into their coronary sinus at the beginning of percutaneous coronary intervention (PCI). Ischemic guidance was done with the WorkMate electrophysiological recording system.
Results: In 11 patients (25%) out of 43 with CHD, the diagonal branch (DB) comprometation and ischemia dynamics (p<0.05) in intracardiac lead (CS 3-4) after ADA stenting were discovered according to ECG-CS. Nine patients (20.9%) underwent successful provisional-T-stenting, while a second stent was required for the other 2 patients.
Conclusion: ECG-CS provides the possibility to optimize coronary intervention in the area of CA bifurcation.
Abbreviations
ADA: Anterior descending artery
BL: Bifurcation lesion
CA: Coronary artery
CHD: Coronary heart disease
DB: Diagonal branch
ECG: Electrocardiography
ECG-CS: Electrocardiography from the coronary sinus
EE: Endocardial electrode
FFR: Fractional flow reserve
iFR: Instantaneous wave-free ratio
MV: Main vessel
MyI: Myocardial ischemia
PBA: Percutaneous balloon angioplasty PCI: Percutaneous coronary intervention RAS: Russian Academy of Sciences
SB: Side branch
Bifurcation stenosis of the coronary arteries is referred to as a “complicated” lesion from the viewpoint of the interventional treatment of CHD, and accounts for 15-20% of the total number of atherosclerotic lesions of the coronary bed (CB) [7,10]. The difficulty in treating the condition is due to the multiple anatomic variants of bifurcation and hemodynamic changes during angioplasty, as these variants make it largely impossible to use the same strategy of interventional treatment for all patients with a bifurcation lesion of CA [7, 10, 12]. The most notable shortcoming of the existing methods of bifurcation stenting is an extensive local “metallization” of a stented artery due to applying one stent to another, in addition to the disturbance of the safety of the polymer- drug layer of stents during operations. These current flaws are often the reasons for restenosis developing and that of arterial bifurcation thrombosis as well, reducing the clinical efficiency of bifurcation stenting in the future [12]. At present, the main strategy of endovascular treatment for most patients with BL is based on stenting in the main vessel (MV) of bifurcation. In the case of optimal results, the dilatation of both branches with the help of kissing angioplasty (provisional T-stenting) is typically used, whereas double stenting methods are used mainly in patients with unsatisfactory clinical angiographical results of the provisional T-stenting (D, F-type dissection, considerable angious pain with negative dynamics of the ECG, bloodstream < TIMI>
Thus, the main problem while choosing the optimal amount of intervention related to BL in most cases is obtaining an objective and exact evaluation of the degree of comprometation of SB ostium after stenting in MV [10]. BL angiography is complicated to perform and interpret due to a number of reasons, such as the complicated geometry of CA, presence of other side branches, intercrossing of vessels, and eccentric growth of atherosclerotic plaque in SB. Nowadays during bifurcational intervention related to CA, to evaluate the functional importance of stenosis of SB, doctors use a method of invasive tests based on the concept of verifying ischemia via analysis of hemodynamic characteristics of intracoronary blood flow in several separate areas of the coronary bed: fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR) [10, 11].
Fractional flow reserve
The method of FFR has some limiting factors in order to be used in clinical practice. Therefore, one FFR measuring elongates the total time of intervention (7 minutes), the efficient dose of radiation (2.8 mSv), and the volume of the introduced radio-opaque contrast agent (35 mL) [17]. Nevertheless, the main limit of using FFR is the necessity of a parenteral injection of vasodilator, as this is related to the risk of developing different side effects such as a sense of heat in the thoracic area, and the induction of life-threatening ventricular disturbances of heart rate [17]. Due to these factors, we do not do FFR for some patients. Thus, in 2017, according to the data given by the American College of Cardiology, doctors in the U.S. evaluated FFR during coronary intervention only in 6.1% of cases [16].
Instantaneous wave-free ratio
The method of detecting iFR cannot be completely validated with the aim of using it as a separate method of detecting myocardial ischemia (MyI) due to the characteristics of coronary blood flow in the area of CA stenosis. In 2020, we still do not have randomized trials where they compare the results of PCI on the basis of functionally evaluating stenosis through iFR to determine intervention tactics using angiographical data and optimal therapy. Likewise, there are very few investigations dealing with the hybrid protocol FFR/iFR, so it is difficult to prove this protocol’s benefits, and the procedures of finding MyI are complicated and elongated, which is why FFR/iFR is rarely used in practice in the catheterization laboratory [11]. Adding to the difficulty, methods of determining iFR and FFR imply complicated and elongated manipulations, and special instruments should be used for CB at different stages of intervention [13, 15].
Electrocardiography from the coronary sinus
A prospective alternative invasive test for optimizing intervention tactics in the area of CA bifurcation is the use of a new electrophysiological method of finding MyI – electrocardiography from the coronary sinus. This method was elaborated, suggested and used by Professor Yu.L. Shevchenko in 2019 at Pirogov National Medical and Surgical Center (The Russian Federation, Moscow) [15]. The exactness of ECG-CS relative to finding ischemia of myocardium during surgical intervention dealing with the major coronary artery has been described by Yu.L. Shevchenko et al. over the course of 2019 and 2020 in some of his articles [13, 14, 15]. According to ROC-analysis done by Yu.L. Shevchenko et al. in 2020, the sensibility of the ECG-CS method in the case of depression arising in ST-segment was 79.5%, with 100% specificity. In the case of registering ST-segment elevation on the intracardiac cardiogram, the sensibility of the method was 83%, with 100% specificity [13].
Fundamental foundation of the possibility of using the ECG method from the coronary sinus to find ischemia of myocardium
From the viewpoint of pathological physiology, coronary stenting of the main vessel with the successive comprometation of the SB ostium is an equivalent of stress for myocardium, due to the fact that cardiomyocytes are not yet ready for acute ischemia. Shifting the ion gradients of cells in the area of hypoperfusion determines the change of the heart’s electric field analyzed by means of an electrophysiologic recording station [2, 4, 8]. According to theoretical and experimental models of the cardioelectric field, the formation of systolic and diastolic flows injuring the myocardium in the case of ischemia can have four possible types of distribution of potential: the rest potential (RP) in the area with ischemia is less (according to module) when compared to the areas with the normal perfusion – hypopolarization; the rest potential in the injured area is higher (according to module) when compared to RP in the area with the normal perfusion – hyperpolarization; action potential (AP) of the pathological area is less when compared to AP of the healthy area –
hypodepolarization; and AP of the injured area is higher when compared to AP of the healthy area – hyperdepolarization. In this situation synergism of the first and third types of potential shifting is possible [2, 3, 4, 5, 8]. Placing an endocardial electrode (EE) into the CS provides the possibility to discover potential differences in the couples of cathode- anode electrodes at the moment of reducing coronary perfusion which is found in intracardiac leads of ECG, such as ST-segment shifting relative to an isoline. The amplitude of deviation is correlated with the degree of ischemia, and the deviation’s direction (depression, elevation) is correlated with the localization of the ischemic center and the charge of the injured area [13]. Thus, we have the aim to evaluate the possibilities of the method of electrocardiography from the coronary sinus to optimize tactics of stenting CA bifurcation lesions.
Study population.
43 patients (100%) who have stable CHD with a pseudo-bifurcation lesion of ADA and without hemodynamically important stenosis of the diagonal branches (DB) have been included in this investigation. For these 43 patients we performed PCI according to the plan between 2018- 2020 at Pirogov National Medical and Surgical Center. All the patients signed an informed consent to take part in the trial. The independence ethics committee of Pirogov National Medical and Surgical Center approved the authors’ desire to hold a trial. The criteria to exclude patients from the experiment were the following: unstable stenocardia, disturbance of heart rate, mitral insufficiency, degree III-IV, disturbance of renal function (creatine >200 mcmol/L), contraindication to have standard antiplatelet therapy, coronary artery bypass grafting in anamnesis, and an occluding lesion of the CA.
Standard functional intraoperation follow-up of a patient’s condition
Doctors performed PCI according to the standard method on the background of a constant follow-up of ECG in three standard leads and in three augmented leads of the extremities of a patient, along with pulse oximetry and the indirect measuring of blood pressure on a 5-10 minute interval with the help of the multiple-parameter configured Datex- Ohmeda Cardiocap 5 monitor (GE).
ECG from the coronary sinus.
The WorkMate (St. Jude Medical) electrophysiological recording system was used in our trial for carrying out invasive intraoperation screening of myocardial ischemia. The catheterization of the CS was done via the subclavical vein by placing a 7F introducer. Under the guidance of X-ray an endocardial 10-canal electrode CS was placed into the CS in the left anterior oblique projection. In order to obtain exact diagnostic results related to myocardial ischemia, we used the bipolar method of the system with the following set up: joining of electrodes into five cathode-anode couples with the frequency range 30-500 Hz, a 1 cm cut-off signal, and amplitude 0.3 mV/cm. The digital analysis of the obtained data was carried out with the EP WorkMate Recording System computer program, version 4.3.2.
Algorithm of performing percutaneous coronary intervention.
During the first stage of intervention, the type of coronary bed lesion (the large diameter of the lateral branches in the area of bifurcation, absence of considerable stenosis of the DB ostium from the viewpoint of hemodynamics before the intervention, the low risk and shifting of atheromatous masses) and constant follow-up on the myocardial ischemia through ECG-CS made it possible to perform stenting of the main branch with the protection of a DB coronary guide wire without additional manipulations for all the patients. Unless angiography discovered
considerable DB stenosis, we performed bifurcation coronary intervention using the method of provisional T-stenting with percutaneous balloon angioplasty (PBA) of DB ostium by means of kissing-dilatation with two balloon catheters. In certain cases, such as if the kissing-dilatation was inefficient, a considerable residual stenosis of the DB ostium was preserved, the blood flow of the side branch was lower than TIMI III, SB dissection type D, F was developing, or there were negative dynamics of ECG-CS, we performed a total bifurcation T- stenting. The stent was placed by means of the coronary guide wire in the diagonal branch, starting from the ostium. The optimization of the stented area was done by means of kissing-dilatation, using two balloon catheters. After PCI the control angiography was performed in at least two orthogonal projections, and then analysis of ischemic dynamics was done. If the ECG-CS results are satisfactory, the instruments are usually removed.
Statistics.
We calculated statistical data using PC MSI by means of Microsoft Excel, and carried out the statistical analysis of data using Statistica 10 for Windows (StatSoftInc., USA). Our aim was to obtain tables, diagrams, graphs and analytical values: the structure (p) of average value (M) and the standard deviation (±sd). Quantitative variables have been described by the following: the number of patients, average arithmetical value (M), a standard deviation from the average arithmetical value, the 25-th and 75-th percentiles, and the median. The difference is considered statistically reliable if the mistake is p<0>
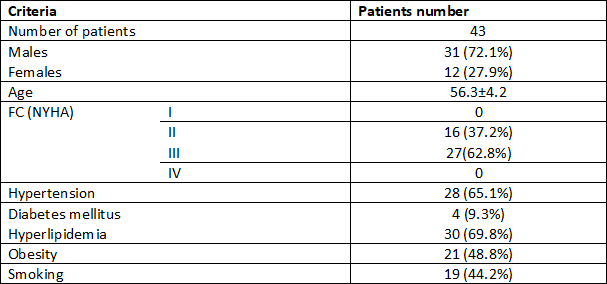
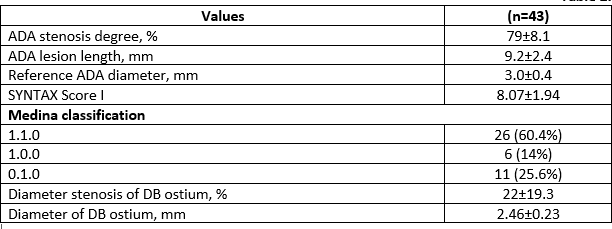
We have made a CHD diagnosis for all 43 patients (100%) as a result of clinical investigation, taking into consideration complaint analysis, anamnesis of disease, and objective methods of investigation. Clinical and angiographic data of patients are presented in Tables 1 and 2.
All the diagonal branches in the BL area are important from the standpoint of hemodynamics: the diameter of the DB ostium is 2.46 ± 0.23 mm. DB stenosis degree is 22±19.3% (Table 2).
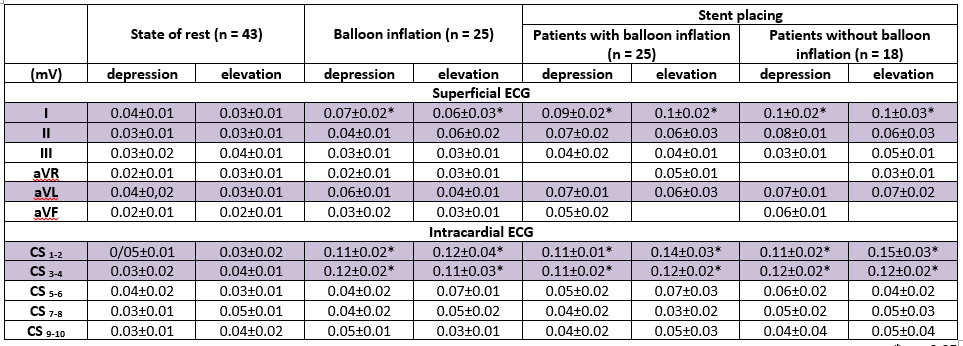
The proper criteria of ischemia, determined through ECG-CS, are the following: ST-segment changes are higher than 0.1 mV. After the electrode was placed into the CS and until instruments were introduced into the coronary bed, we did not observe any ischemic changes (p=NS). In Table 3, the dynamics of ST-segment during intervention into the ADAin the area of bifurcation are shown. During balloon inflation and ADA stenting using an endocardial electrode, the ischemic dynamics (p<0>Table 3).
After ADA stenting for 32 patients, although there had been angiographic signs of exacerbating stenosis of the DB ostium, ischemic changes were not registered in the superficial ECG and ECG-CS. Thus, we decided to
stop PCI. In 11 patients after ADA stenting ischemic dynamics (p<0>Table 4).
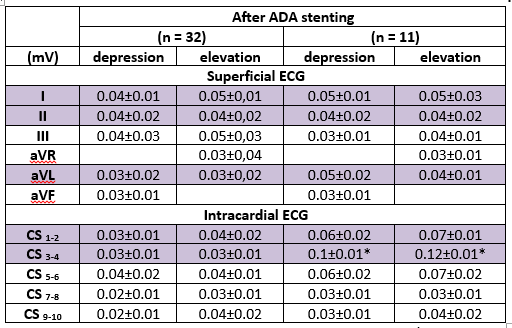
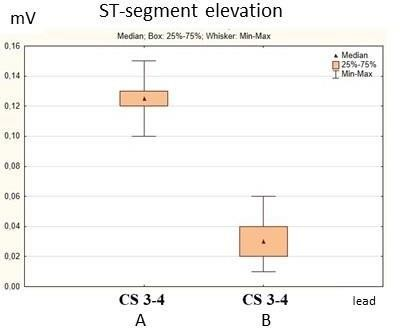
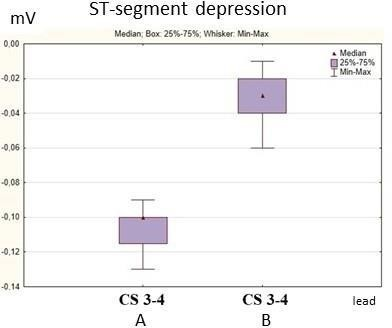
The minimal depression in CS 3-4 lead was 0.09 mV, the maximal depression 0.11 mV, and elevation 0.1 mV and 0.15 mV, respectively (A). In 32 patients we did not find ischemic changes to the ST-segment (B).
The maximal depression, found in CS 3-4 lead, was 0.06 mV, and the maximal elevation was 0.06 mV (Figures 1 and 2).
Taking several things into consideration, such as the clinical presentation, the angiographic data of worsening DB stenosis, and the ischemic
changes in the intracardiac ECG, we decided to perform T-stenting of the DB ostium with PBA by means of the kissing-dilatation method (Table 5).

After PBA of the DB ostium, done by the standard method and according to intracardiac ECG, ischemic changes were not registered for 9 patients (p=NS). In 2 patients, despite angioplasty of the LB ostium, angiographic signs of residual stenosis of the SB and depression in CS 3-4 led up to
0.12 mV and the patients experienced pain in the retrosternal area. We thus decided to perform the total T-stenting of the DB. After the operation, the dynamics of the ST-segment were not registered in 11 patients.
After coronary stenting, none of the patients complained about stenocardia; when hemostasis occurred, we transferred all the study’s patients into the intensive care ward for a day to allow for dynamic follow-up. During their time in intensive care, every patient’s condition was evaluated as stable, in regards to functional (the standard dynamic ECG in 12 leads) and clinical criteria. Angiography was not required. After one day, each patient was transferred back to our department.
The most pertinent problem of PCI in the area of bifurcation when using the method of stenting with a double-guide-wire technique and provisional T-stenting is evaluating the functional importance of the SB for myocardium. The hemodynamic importance of ostium stenosis, unaccompanied by either reliable ischemic changes according to a standard ECG or if blood flow is lower than TIMI III, has not yet been determined. The problem of whether balloon angioplasty should be performed or not remains difficult. On one hand, it is necessary to acknowledge angiography’s limitations, which often result in an underestimation of the stenosis, while on the other hand, we should keep in mind the dissection risk and a successive and necessary transition to PCI with double-stenting, which increases the risk of SB restenosis in the future [7, 10,12]. FFR and iFR methods used nowadays to optimize the tactics of coronary intervention have a number of limiting factors and restrictions [11, 17]. The perspective alternative to invasive stress tests is introducing the method of ECG from the coronary sinus in order to determine the optimal volume of coronary intervention in the area of CA bifurcation [13, 14, and 15]. In the area of ADA blood supply, reliable dynamics of ST-segment during intervention were registered in the CS 1- 2 lead and in the CS 3-4 lead of the endocardial electrode. During the blocking of blood flow, the minimal ST-segment shifting according to the module was 0.09 mV, and the maximal shifting 0.2 mV. We did not find
a difference in amplitude of the ST-segment in patients with pre-dilatation of stenosis and in those patients who had direct coronary stenting.
The results we obtained during this study completely correspond to the results of the trial held by Yu.L. Shevchenko et al. (2019, 2020), and they confirm the positive results of the use of ECG-CS [13, 14, 15]. The intracardiac CS 3-4 lead bears responsibility for the ischemic dynamics in the area of blood supply of the diagonal branch of the ADA, and corresponds to the topographic characteristics of the coronary sinus and the topic of the myocardial perfusion of the diagonal branches of the ADA [13].
The results of our trial (taking the exactness of ECG-CS relative to ischemia of myocardium in case of comprometation of the side branch of CA into consideration) also correlate with the data we have seen in global medical literature. In his article, Ahn J. et al. (2012) mentioned that in patients having CHD with BL (stenosis of SB before the operation was in 34.8±17.8% of cases), 17.8% of lateral branches had hemodynamically reliable stenosis of BL according to FFR after MV stenting [1]. In the trial conducted by Kang S.J. et al. (2013), Kang noted that after the coronary stenting of the main vessel in patients with BL (SB stenosis before the operation was in 24.8±16.0% of cases), 15% of their lateral branches required additional intervention on the basis of FFR index [9].
In our trial, the use of ECG-CS gave us the possibility to avoid additional intervention in 32 (74.4%) patients who had CHD with MV stenting, having SB protection by a guide wire. In patients who had DB comprometation, the use of the data from intracardiac ECG was helpful to determine the necessary volume of coronary intervention: for 9 patients (20.9%) we performed provisional T-stenting; in 2 (4.6%) patients we found indicators to use a double-stenting method of PCI.
The ECG-CS method has an exactness relative to myocardial ischemia with invasive loading tests in the case of bifurcational interventions related to pseudo-bifurcation lesions of CA [1,9]. Additionally, the ECS- CS method does not have limitations that are typical to FFR and iFR [13].
Therefore, we can say that this brand new approach to determining stenting tactics of bifurcational lesions of CA using ECG-CS is effective.
There are no limitations related to the investigation.
It is recommended to use the ECG-CS method in the case of coronary intervention in the area of CA bifurcation if you have the necessary equipment with the described modes.
The diagnostic criteria of ischemia in the area of blood supply of the ADA diagonal branch is the depression or elevation of the ST segment more than 0.1 mV in the intracardiac CS 3-4 lead of a standard 10-canal electrode.
Electrocardiography from the coronary sinus is a new and efficient method of optimizing tactics of percutaneous coronary intervention in the area of bifurcation of coronary arteries.
ECG-CS provides the possibility to determine the degree of SB comprometation in the area of CA bifurcation using a single- stent approach to PCI in patients with stable CHD who have relative indicators.
The use of the ECG-CS method provides the possibility to discover patients with coronary atherosclerosis when the area of CA bifurcation has a lesion and when it is not possible to avoid the transition to a double-stenting PCI method.
The authors have confirmed the absence of relations that could be interpreted as conflicts of interest.
This investigation has not received any grant from the governmental, commercial or non-commercial sector.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
